Strabismus (crossed eyes & wandering eyes)


On this page
What is strabismus?
Strabismus types
Signs and symptoms of strabismus
What causes strabismus?
Possible complications
How is strabismus diagnosed?
Can you prevent strabismus?
Strabismus treatment
Outlook for strabismus
When to talk to an eye doctor
On this page
What is strabismus?
Strabismus types
Signs and symptoms of strabismus
What causes strabismus?
Possible complications
How is strabismus diagnosed?
Can you prevent strabismus?
Strabismus treatment
Outlook for strabismus
When to talk to an eye doctor
What is strabismus?
Strabismus is the medical umbrella term for all types of eye misalignment. Some more familiar terms include crossed eyes, squint or wandering eyes. Strabismus is very common and can be present at birth or begin later on. Untreated, it can lead to amblyopia (lazy eye) and long-term vision conditions.
It’s normal for newborns to have trouble focusing for their first few months. Sometimes, this can look like strabismus, but their focus will typically get stronger by 3 to 6 months of age. Even so, make sure to schedule a pediatric eye exam if you notice any issues.
Around 3% to 4% of people have some form of strabismus, with around 33% of cases developing by 8 months of age.
Strabismus types
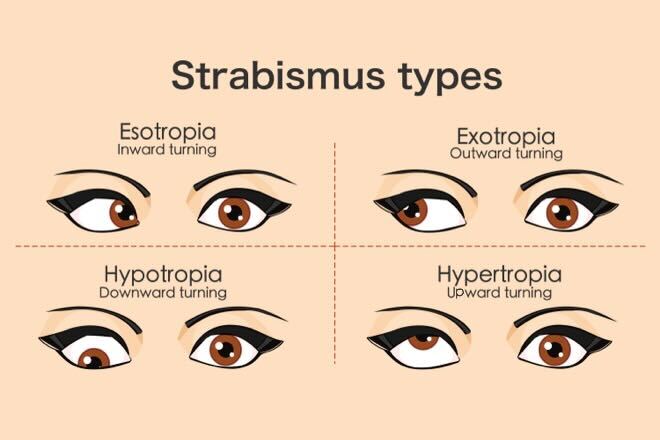
There are several different types of strabismus. They are often categorized by the direction and duration of the eye’s misalignment. For example, it may be horizontal or vertical:
- Esotropia – The misaligned gaze is toward the nose.
- Exotropia – The misaligned gaze is away from the nose.
- Hypertropia – The misaligned gaze is upward.
- Hypotropia – The misaligned gaze is downward.
Some types of strabismus are present all the time (called constant). Others are only present sometimes (called intermittent). Strabismus can also be categorized by when it develops, what caused it and other factors.
The type of strabismus a person has is a combination of all the factors. Some of the more common types of strabismus include:
Accommodative esotropia
This type of strabismus develops when a child needs to use excessive effort to focus up close. It is more common in children who have moderate to high farsightedness. On average, the age of onset is about 3 years old, but it can be earlier or later. It can occasionally develop in adults with presbyopia as well.
Often, accommodative esotropia can be corrected with eyeglasses or contact lenses.
Intermittent exotropia
In this type of strabismus, one eye will turn outward, but only sometimes, and not always the same eye. It usually happens when focus is relaxed, such as when very tired, daydreaming or looking at something far away.
This is the more common type of strabismus overall. It begins sometime between birth and 2 years old as an exophoria. This means, at first, it only happens when one eye is covered. Eventually, it can progress to intermittent exotropia.
Eyeglasses, vision therapy and eye patching can improve the condition for some people. However, many need surgery to improve it or to keep it from progressing to a constant exotropia.
Infantile esotropia
Strabismus is called infantile if it occurs within 6 months to 12 months after birth. It’s not the same as congenital, which means present at birth. It’s also not the same as the normal difficulty with focusing that all newborns have.

Infantile esotropia is a constant crossing of one or both eyes. In the majority of cases, the amount of deviation (called the angle) is obvious, and it stays the same all the time.
Many babies who have infantile esotropia need strabismus surgery. However, in mild cases, a series of botulinum toxin injections combined with eyeglasses and patching may work to straighten the eyes.
READ MORE: Infant vision development
Other ways to classify strabismus
There are many other ways a pediatric ophthalmologist or optometrist may classify strabismus. If you or your child see an eye doctor about strabismus, things they may talk about include:
- Large-angle vs. small-angle – This refers to the amount or degree of misalignment. Large angle typically means 30 “prism diopters” or more.
- Unilateral vs. alternating – Unilateral means it only happens in one eye. Alternating means it can switch back and forth between each eye.
- Latent vs. manifest – Latent means it only happens when one eye is covered (like esophoria). Manifest means it’s present all the time.
- Comitant vs. incomitant – Comitant means the degree of misalignment between the eyes never changes. Incomitant means it might lessen or get worse, depending on the direction of the eyes.
- Pseudostrabismus – This is “false” strabismus. Some babies’ eyelids cover enough of the inner corners of the eyes that it looks like they have crossed eyes. It’s harmless, and they will typically grow out of it with time.
- Convergence insufficiency – This is an eye movement disorder that can lead to strabismus.
Signs and symptoms of strabismus
The primary sign of strabismus is a visible misalignment of the eyes. One eye turns in, out, up or down. The other eye looks directly at the object being viewed.
If your child has strabismus, you might notice they cover one eye when looking at something close up or far away. They may also tilt or turn their head to try to focus. They may have difficulty with reading, eye-hand coordination and tasks that use depth perception.
Symptoms of strabismus can vary, depending on a person’s age and type of strabismus. In older children and adults, symptoms can include:
- Double vision (diplopia)
- Eye strain (asthenopia)
- Loss of depth perception
- Sensitivity to bright light (photophobia)
- A feeling of weakness or “pulling” in your eye
- Headaches
Younger children may not realize or be able to vocalize that they have these symptoms. When eye and vision problems begin very early, children often aren’t aware that there is anything wrong or different.
In addition, their brains can suppress, or hide, the vision problems caused by strabismus. This is what can eventually cause them to develop amblyopia (lazy eye).
What causes strabismus?
Each eye has six external muscles called the extraocular muscles. They work with the brain and nerves to control eye position and movement. For normal binocular vision, the muscles, nerves and brain must work together correctly for both eyes.
Strabismus occurs when there are problems with the muscles that control the eyes. Sometimes the problem is anatomical (in the muscles themselves). Other times, it is neurological (in the nerves or the part of the brain that controls binocular vision).
In many cases of infantile and early childhood strabismus, the exact cause of these conditions is unknown. But in older children and adults, it’s often related to other health conditions, including:
- Moderate to extreme farsightedness or nearsightedness
- Much poorer vision in one eye than the other
- Retinal abnormality
- Cerebral palsy
- Down syndrome
- Head injury
- Brain tumor
- Stroke
- Graves’ disease
- Guillain-Barré syndrome
- Cranial nerve palsy
Children are also more likely to develop strabismus if they have a low birth weight or other family members with strabismus.
READ NEXT: Brushfield Spots
Possible complications
The more serious problem caused by strabismus is another eye condition called amblyopia.
When the eyes can’t work together, they send two images to the brain (double vision) instead of one. To try to maintain good vision, children’s brains can learn to ignore one of the images.
But since their vision is still developing, this means they can never develop good vision in that eye. When vision stops developing in that eye, it’s called amblyopia (or lazy eye).
How is strabismus diagnosed?
Routine children’s eye exams are the optimal way to detect strabismus. Generally, the earlier strabismus is treated, the more successful the outcome. Without treatment, it can cause double vision, symptoms that interfere with learning and amblyopia. Amblyopia can lead to permanent decreased vision if it isn’t corrected by age 5 to 8.
Some of the tests the eye doctor may use to diagnose strabismus include:
- Corneal light reflex test – This test evaluates eye alignment based on the location of reflections of light shined at the eyes.
- Visual acuity test – They may use a Snellen chart or a special chart for children.
- Cover/uncover tests – They may do a variety of tests that involve covering the eyes one at a time. This helps them determine when and how much an eye might turn.
- Depth perception tests – They may use a viewing instrument or cards with special images that help assess 3D vision.
- Ophthalmoscopy – They will dilate the pupils and use a special microscope and bright light to look inside the eye. This helps them determine whether it’s amblyopia or something else causing the vision loss, as well as look for causes of strabismus.
- Brain and eye imaging – For later onset strabismus, they may need to check for neurological or eye muscle disorders that may be causing it. This includes testing for thyroid eye disease, which involves extraocular muscle imaging (usually with ultrasound).
Can you prevent strabismus?
Strabismus itself can’t be prevented. However, amblyopia, vision loss and other vision conditions can often be avoided with prompt treatment.
Strabismus treatment
Pediatric ophthalmologists and optometrists will usually try non-surgical treatment first, if possible. Surgery is the first line of treatment in some cases.
Non-surgical strabismus treatment
In some cases, it may be possible to improve eye alignment non-surgically. These treatments can include eyeglasses, eye patching, vision therapy and even botulinum toxin injections. Refractive correction by itself or corrective lenses with prism can also be used as a non-surgical option.
However, they may only be helpful in milder cases. Eye doctors may recommend them for intermittent and small-angle strabismus, or when it’s related to poor vision.
For babies and very young children, doctors may use special eye drops as a temporary treatment.
Strabismus surgery
Often, the only effective treatment is strabismus surgery. There are many different types of surgery, but many involve the eye muscles. The surgeon may strengthen, weaken or adjust certain eye muscles, depending on the type of strabismus you have.
In some cases, the eye may need more than one surgery. The surgeon may also recommend eyeglasses, patching, vision therapy or botulinum toxin injections post-surgery.
Strabismus surgery can also be effective for adults with long-standing strabismus. Often, however, a significant degree of amblyopia remains after the surgery. This is why early treatment of strabismus is so important.
Outlook for strabismus
Early diagnosis and treatment usually have excellent results. The earlier a child is treated for strabismus, the more likely it is that they can develop normal vision.
Children often need treatment by 6 months to 3 years of age to avoid permanent vision conditions. This is just one reason why it’s important to make sure your child has pediatric eye exams.
When to talk to an eye doctor
When talking with your eye doctor or strabismus surgeon about treatment, here are a few important questions to ask:
- If surgery is recommended, ask whether you will need one surgery or if additional procedures may be necessary.
- Ask about the success rates for the type of strabismus treatment they are recommending.
- Ask how they determine if the treatment is a success. Is “success” defined as reducing the eye turn so the eyes look more natural? Or, is success defined as eyes with normal visual acuity, eye teaming and depth perception?
- Ask about the success rate, duration and costs of vision therapy.
- Ask how much of the costs for strabismus treatments are covered by health or vision plans.
Remember, children do not outgrow strabismus. Seek treatment for strabismus as soon as possible to prevent permanent vision conditions.
READ NEXT: Can a head injury cause crossed eyes?
Judith Lee and Gretchyn Bailey also contributed to this article.
On this page:
What is strabismus?
Strabismus types
Signs and symptoms of strabismus
What causes strabismus?
Possible complications
How is strabismus diagnosed?
Can you prevent strabismus?
Strabismus treatment
Outlook for strabismus
When to talk to an eye doctor
On this page:
What is strabismus?
Strabismus types
Signs and symptoms of strabismus
What causes strabismus?
Possible complications
How is strabismus diagnosed?
Can you prevent strabismus?
Strabismus treatment
Outlook for strabismus
When to talk to an eye doctor